
Photo: alikemalkarasu / E+ / Getty Images Plus
One of the top search phrases on SkinCancer.org is, “Can I leave my skin cancer alone?” Two of our physician experts answer why, when you’ve been diagnosed with a skin cancer, time is of the essence.
Timing is crucial in treating skin cancers, but is it more so with some types than with others? Let’s start with the less common but more dangerous type: melanoma.
Julie K. Karen, MD: Melanoma is in a class by itself, and it’s important to be clear and unequivocal: Absolutely under no circumstances should you leave melanoma alone. A recent study in JAMA Dermatology found that melanoma patients treated within 30 days of the biopsy had a better outcome than those who waited. Waiting increased the risk of death. And, in that vein, if you have any reason to suspect that you or a loved one may have melanoma, you don’t want to wait six months to have it examined, because of how rapidly melanoma can progress.
Leonard H. Goldberg, MD: While there are various stages to grade melanomas, they basically fall into two main categories when it comes to timing: before they metastasize (spread) and after they metastasize. If you cut them out before they metastasize, there’s a good chance the patient is cured. If you get them after they metastasize, it’s a whole different ballgame. And you can’t second-guess or predict the crucial moment in time when that melanoma changes from one category to the other. It’s like gambling with your life.
If you see someone and suspect melanoma, do you hint at it then, or do you always wait for the biopsy results?
Dr. Karen: I do hint at it. I don’t want to ruin someone’s day or weekend when I might be wrong, but, at the same time, I don’t feel it’s right to have a patient be absolutely floored if diagnosed with melanoma. I express concern and justify why the biopsy should be done immediately. I do the biopsy that day, and I would never let the patient put it off. Once the diagnosis is confirmed, the goal is to treat it as quickly as possible.
Dr. Goldberg: I say to the patient, “I need to remove this. It’s a suspicious pigmented lesion (meaning it’s dark in color), and it’s got to go.” Most melanomas are pigmented. The rare ones that are not pigmented are a dermatologist’s nightmare, because they may look like something benign. By the time you figure out it is a melanoma, you may have lost the ballgame.
A recent study found that melanoma patients treated within 30 days of the biopsy had a better outcome than those who waited. Waiting increased the risk of death.
What about timing with basal cell carcinomas (BCCs), the most common type of skin cancer?
Dr. Goldberg: If it’s a basal cell carcinoma, it comes off. I’d never wait to do treatment, because tumors grow all the time — sometimes slowly, but not always. I did a study that showed that the time between when someone is first diagnosed and when you remove the skin cancer makes a huge difference. Death from BCC is extremely rare, but large ones can disfigure your face, affect movement and function — and leave large scars.
Dr. Karen: Yes, people have a tendency to think that because BCCs are slow-growing, they can wait on treatment, or even blow it off. For those who have high deductibles, cost very often is a factor. However, early detection through regular skin exams can keep the treatment minimal and the cost as low as possible.
If you wait until a BCC is bothersome, cosmetically or symptomatically (for example, if it’s bleeding frequently), it’s a much bigger deal to treat at that point. BCCs often have “roots” underneath the skin, so what’s below the surface could be larger than what meets the eye. The surgery to remove those can be far more disfiguring.
How do you answer a patient who begs for permission to wait on surgery for a BCC till after a big event? For example, “My daughter is getting married in a month. Can we do this surgery on my face after that?”
Dr. Karen: It’s hard to say, because not all BCCs are created equal. I would always rather treat it sooner than later, because it could be growing under the skin, resulting in a much larger scar than we would anticipate. But, if you have a major life event that you need to put it off for, and you want to wait a month or two because your daughter’s wedding is coming up, that might be acceptable for a BCC. But not for a melanoma, which we talked about earlier, or a squamous cell carcinoma (see below). You should always be under the care of a physician, and if that lesion is rapidly growing, you should not wait.
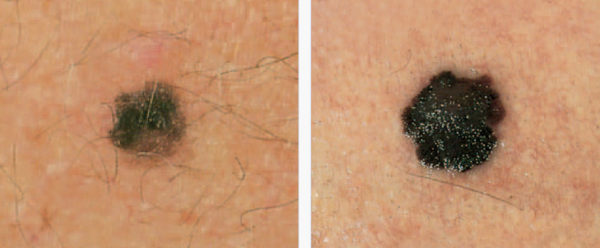
E Is for Evolving – A melanoma, like the one above, can grow outward, upward and inward in a matter of months.
What about squamous cell carcinoma (SCC), the second most common form of skin cancer? Can patients leave those alone for a while?
Dr. Goldberg: The simple answer is no. People lump basal cell and squamous cell carcinomas together as “nonmelanoma skin cancers,” but that’s doing them a disservice. They’re not the same. I lose two patients a year to advanced squamous cell carcinoma. While it’s hard to get exact numbers because tumor registries don’t track SCCs, the latest figures suggest that in 2021, more than twice as many people (over 15,000) will die from SCC in the U.S. than from melanoma (7,180). With SCCs, we don’t wait.
My cousin asked my advice about a friend living in South Africa who was diagnosed with an SCC on his scalp. I said to my cousin, “Tell him to get on a plane tomorrow and come see me. I will take care of him, I will remove it and he will have a good life.” Instead, the man waited, then went to a doctor in South Africa and was treated with radiation. The cancer returned, and it had spread into the skull. Within two years, he was dead.
Dr. Karen: SCCs can metastasize to the local lymph nodes, even to some organs, and can become deadly. Thankfully, it’s rare. The people who are most at risk of dying from SCC are the very old or those whose immune systems are suppressed because of antirejection drugs after a transplant, or patients who are on immunosuppressive medication for their psoriasis, psoriatic arthritis or other conditions. But it can happen to others, too.
Dr. Goldberg: Be aware of lesions that are painful or associated with numbness or other neurological symptoms. That could be a red flag that it has gotten close to or invaded a nerve, and you really want to get that checked out. It can be a sign of invasive skin cancer. My best advice overall? Just treat your skin cancers early.
Do the same rules apply for older people?
Some news articles have suggested that older people may be overtreated for skin cancers that might grow slowly and probably never kill them. But how do you justify not treating someone who has skin cancer?
Dr. Goldberg: I never tell someone that he or she is too old for skin cancer treatment. If not treated, tumors can grow, ulcerate, bleed and become infected and painful. That becomes a problem for the patient, the family and caregivers. I have found removal of these tumors to be safe and effective — and a relief to all.
Dr. Karen: I favor treating, and this is nonnegotiable when it comes to melanoma. It’s much less of a big deal to take care of a skin cancer when it’s tiny and curable rather than allowing it to grow, when treatment can be far more extensive and can lead to complications. If the patient is in reasonable health and is reasonably expected to live three to five years or more, I would treat most skin cancers aggressively.
If a person’s life expectancy is between two and five years, we usually have a candid discussion about all the options. But, generally, I’m on the side of treating with those patients, too. Treatment can improve quality of life.
If a patient has serious health issues and a life expectancy of less than two years, then you have to have a discussion with the family. Then it may be hard to justify treating a basal cell carcinoma in those patients. If it’s a squamous cell carcinoma, it’s tricky. I’d prefer to treat it, but if the person is too sick to have a surgical procedure, the person or family may not want to risk it. But I still have a hard time not treating people.
Dr. Goldberg: I have treated many 90-year-old patients and also centenarians and two patients aged 104. People are living longer and healthier lives. It is almost impossible to prognosticate when someone will pass on. Data show that older people who are treated for skin cancers have a better longevity.
Leonard H. Goldberg, MD, is a leader in Mohs micrographic surgery at DermSurgery Associates in Houston, and author of more than 200 publications on the subject. He is a staff member of Houston Methodist Hospital, and a vice president of The Skin Cancer Foundation.
Julie K. Karen, MD, is a Mohs surgeon and specializes in the diagnosis and treatment of skin cancer at CompleteSkinMD in New York City. She is also a clinical assistant professor in the Ronald O. Perelman Department of Dermatology at NYU Langone Medical Center.
![]()
*Last updated: Jan 2021